

About Implantable Devices
If your hearing loss cannot be treated effectively by hearing aids, you may be a candidate for one of three types of implantable devices:
- Cochlear implant – Most often used for people with severe-to-profound sensorineural hearing loss
- Bone conduction hearing device – Intended primarily for conductive or single-sided hearing loss
- Middle ear implant – Sometimes recommended for those with mild-to-moderate hearing loss who would benefit from hearing aids but cannot wear ear molds
The surgical procedures required by these options are generally considered to be quite safe. It can help to discuss any concerns with your doctor and speak to implant recipients about their experiences.
What is a cochlear implant?
 Your cochlea is a snail-shell shaped organ in the inner ear lined with cilia, delicate hair-cell nerves that enable hearing. When these tiny cells become irreversibly damaged, it results in sensorineural hearing loss.
Your cochlea is a snail-shell shaped organ in the inner ear lined with cilia, delicate hair-cell nerves that enable hearing. When these tiny cells become irreversibly damaged, it results in sensorineural hearing loss.
For most people with hearing loss that involves the inner ear, the auditory nerve itself still works, even though the hair cells no longer function. A cochlear implant (CI) transforms acoustic sound signals into electric stimuli, bypassing the damaged cilia and sending them straight to the nerve.
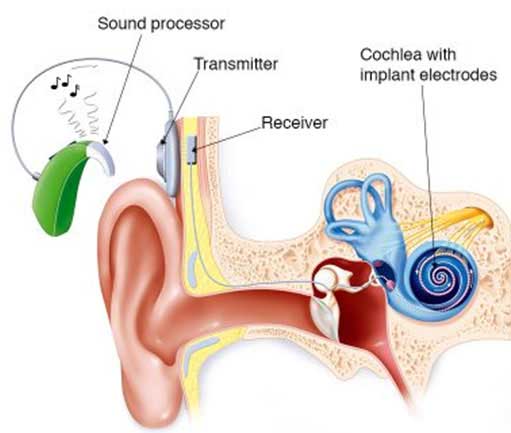
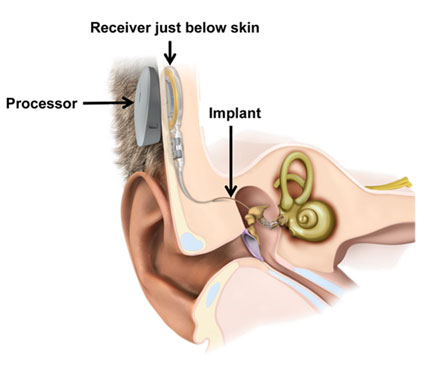
A CI is a small electronic device with four internal and external components:
- Sound processor with microphone
- Receiver implanted under the skin
- Transmitter attached with a magnet
- Electrode array inserted into the cochlea
Who can benefit from a cochlear implant?
Children and adults with significant hearing loss are candidates for cochlear implants. Regardless of age, experts recommend that implantation occur as soon as possible to receive the most benefit. In children, this may be critical for the development of speaking, reading and social skills.
Eligibility for a cochlear implant begins with a comprehensive evaluation and testing, generally by an otolaryngologist (ear-nose-throat doctor, or ENT), often in conjunction with an audiologist. Most candidates have difficulty understanding spoken communication, even with hearing aids.
Over the past 50 years, close to one million cochlear implants have been implanted worldwide. Read real-life stories of people who have been helped by cochlear implants here.
How a cochlear implant can help
While it cannot restore normal hearing, a CI may help someone with significant or complex hearing loss to receive sounds and better understand speech. Guidelines for CI candidates have expanded to include an array of hearing loss levels for adults and children, and CI’s may be used in conjunction with other devices for better results.
A CI recipient may experience:
- Increased ability to understand speech and hear conversations
- Reduction in tinnitus (noise or ringing in the ears)
- Enhanced safety
- Improved communication and relationships
- Richer engagement with the world
For best results, CI recipients often do aural rehabilitation after surgery to retrain the brain and learn to interpret the signals enabled by the device.
While a CI helps sound to bypass a damaged cochlea, other implantable devices that bypass the middle or outer ear are used as alternatives to conventional hearing aids for those who can’t wear them.
Bone conduction hearing devices
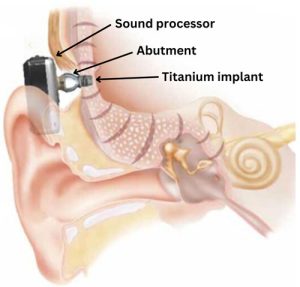 Bone conduction hearing devices, also called bone-anchored hearing systems, may be an option if outer or middle ear issues such as a collapsed ear canal or frequent ear infections prevent you from wearing conventional hearing aids.
Bone conduction hearing devices, also called bone-anchored hearing systems, may be an option if outer or middle ear issues such as a collapsed ear canal or frequent ear infections prevent you from wearing conventional hearing aids.
- Can help provide amplification for people with conductive or mixed hearing loss
- The implant connects to a tiny titanium stud that’s anchored to the skull and connects to a processor worn behind the ear
- When the microphone picks up incoming sounds, the processor transmits them to the inner ear through acoustic vibrations
Middle ear implants
 Middle ear implants are a newer solution for those who cannot wear ear molds due to allergies, infections, skin conditions, narrow or blocked ear canals or misshapen ears.
Middle ear implants are a newer solution for those who cannot wear ear molds due to allergies, infections, skin conditions, narrow or blocked ear canals or misshapen ears.
- Suitable for those with mild-to-moderate conductive, sensorineural or mixed hearing loss
- A small, wire-like piece is attached to one of the bones in the middle ear
- Rather than amplifying sound to the eardrum (as a hearing aid does), an MEI mechanically stimulates the middle ear bones and transmits sound to the cochlea